Macular Degeneration Foundation
EyeSight.org

How Does Red Light Therapy Affect Eyesight?

By: Anna Barden, Writer
For: All About Vision
Red light therapy is popularly used to improve the feeling and appearance of the skin. It promises to treat acne, wrinkles, scarring and even signs of aging on the face — but can it protect aging eyes? Some studies say yes, but researchers are still trying to understand the benefits.
What is red light therapy?
Red light therapy involves exposing the skin to red light-emitting diode (LED) light to target unwanted skin features such as acne, wrinkles and age spots. This is done using devices such as LED masks (also called light therapy masks). However, at least one LED mask model has been recalled due to concerns over eye safety.
Research has found that different types of light hit the skin at different depths. For example, red LED light triggers special skin cells called fibroblasts, which produce collagen — the protein that aids in the recovery of damaged skin.
While red light therapy is most commonly used for repairing blemished skin, other studies have suggested that it may also improve eye health. While FDA-authorized light therapy systems exist for certain eye conditions, such as dry age-related macular degeneration (AMD), these clinical devices can only be used under medical supervision.
Red light therapy for eye health
A quick online search on “how to use red light therapy for eyes” may present several procedures and reasons for using them. You may come across things such as red light therapy for dry eyes or red light therapy for retina health.
Here’s what the latest research shows:
Red light therapy for dry eyes
Those who struggle with dry eyes due to meibomian gland dysfunction (MGD) may benefit from red light therapy, according to some studies. In one clinical trial, researchers looked at whether low-level light therapy (also called photobiomodulation or PBM) could help people with dry eye disease. Adults with dry eye received a series of LED light treatments around the eyes over several weeks, while another group received a placebo treatment.
After four weeks, people who had the light therapy showed improvements in symptoms, tear production, and certain signs of eye surface health. The study found these benefits occurred without serious side effects, suggesting that low-level light therapy might be a safe and helpful option for improving dry eye symptoms.
Another trial found that low-level light therapy treatment improved symptoms of dry eye. While these are promising results, additional studies are still needed to understand the potential benefits and risks.
Red light therapy for retina health
Located at the back of the eye, the retina and its photoreceptors (the rods and cones that sense light and color) are especially susceptible to the effects of aging. So, can red light eye therapy protect your vision long-term?
Research suggests that light therapy may help by improving how retinal cells produce energy and by reducing harmful changes in the eye. In clinical studies, people with early-to-intermediate dry age-related macular degeneration who received light therapy showed promising results:
* Less progression toward severe vision loss
* Fewer drusen (the waste deposits that build up in AMD)
* Improved vision on eye charts (in some cases)
This approach is FDA-authorized for patients with early-to-intermediate dry AMD, but it’s not a cure and it’s currently performed only under the supervision of an eye care professional. It has not been studied or cleared for wet AMD.
Light therapy for AMD is non-invasive and usually painless, taking only a few minutes per eye in a medical setting. Researchers are still learning more about which patients benefit most and how often treatment should be repeated.
Red light therapy for glaucoma
Recent studies have explored the effects of red light therapy for glaucoma, such as photobiomodulation therapy, but it is not yet a standard glaucoma therapy. Research in this area is ongoing. Scientists are still working to better understand who may benefit most and how these treatments should be used in the future.
Is red light therapy safe for my eyes?
Despite positive findings, ophthalmology experts say there’s not enough research to prove that using red light therapy around the eyes is 100% safe and effective for everyone. Since things are uncertain, it’s important to take precautions before beginning any red light treatments, whether at home or in a doctor’s office.
Until more research is done, consider that there may be risks in red light exposure. And always talk to your eye doctor before beginning any kind of treatment on your eyes.
For the time being, be sure to protect your eyes from known harmful light sources such as ultraviolet (UV) rays, and don’t forget to schedule your yearly comprehensive eye exam.
What is Glaucoma?
Edited Abstract from Encyclopedia.com
Description
Between two to three million people in the United States have glaucoma, and 120,000 of those are legally blind as a result. It is the leading cause of preventable blindness in the United States and the most frequent cause of blindness in African-Americans, who are at about a three-fold higher risk of glaucoma than the rest of the population. The risk of glaucoma increases dramatically with age, but it can strike any age group, even newborn infants and fetuses.
Causes
The cause of vision loss in all forms of glaucoma is optic nerve damage. There are many underlying causes and forms of glaucoma. Most causes of glaucoma are not known, but it is clear that a number of different processes are involved, and a malfunction in any one of them could cause glaucoma. It is probable that most glaucoma is inherited. At least ten defective genes that cause glaucoma have been identified.
Treatment
When glaucoma is diagnosed, drugs are typically given as eye drops. There are also several types of laser surgery used to treat glaucoma. Microsurgery (or “filtering surgery”) has been used in many different types of glaucoma. These surgeries are usually successful, but the effects often last less than a year.
Prognosis
About half of the people stricken by glaucoma are not aware of it. For them, the prognosis is not good, and many of them will become blind. Sight lost due to glaucoma cannot be restored. On the other hand, the prognosis for treated glaucoma is excellent.
Prevention
Because glaucoma may not initially result in symptoms, the best form of prevention is to have regular eye exams.
=========
Resources:
1. Amazon Book: There’s No Vision Like Low Vision by Tom Perski
2. Exclusive Video: Wearable low vision devices designed for people with macular degeneration and glaucoma.
Invitation to Research Study

LaGrippe Research, a market research firm specializing in healthcare, is working on a project on the topic of Age-related Macular Degeneration and/or Diabetic Macular Edema and are inviting patients who have been diagnosed and/or their care partners to participate. Should this apply to you, please see below for details.
This will be in the form of a 45-minute online discussion. Those that qualify and participate will be compensated $125 as a thank you. The dates available for this discussion are June 8th – August 3rd. Participants must live in the USA.
If you are interested, please fill out our preliminary questions online here: https://lagripperesearch.research.net/r/K8QGB7F
If you have any questions, please contact Alex at 847-533-4052 or alex@lagripperesearch.com
Mobility for Low Vision
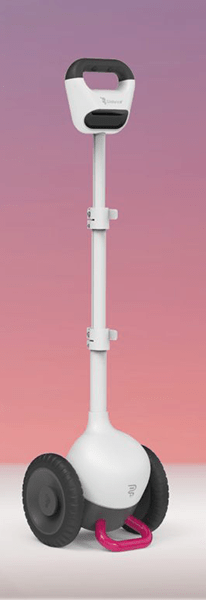
“Glide” is designed to assist blind and low vision individuals to navigate outdoor and indoor environments safely and independently.
- Avoid obstacles & hazards
- Find doors, elevators, stairs, & more
- Navigate any terrain
- Pre-mapped and freestyle walking
For more information:
Glidance Website
Vision with Artificial Intelligence

EYEDAPTIC.com
Vision enhancement and visual assistance with the EYE7
Improve vision for those suffering from retinal disorders including AMD (age related macular degeneration) through the development of software driven smart glasses, leveraging the power of augmented reality (AR) and artificial intelligence (AI) technology.
Strategy to Prevent ARMD
Washington University School of Medicine
Fixing problems in cholesterol metabolism could stave off a leading cause of blindness, according to new research in mice, human plasma samples
A new study from Washington University School of Medicine in St. Louis identifies a possible way to slow or block progression of age-related macular degeneration, a leading cause of blindness in people over age 50. The WashU Medicine researchers and their international collaborators implicated problems with cholesterol metabolism in this type of vision loss, perhaps helping to explain the links between macular degeneration and cardiovascular disease, which both worsen with age.
The new findings — identified using human plasma samples and mouse models of macular degeneration — suggest that increasing the amount of a molecule called apolipoprotein M (ApoM) in the blood fixes problems in cholesterol processing that lead to cellular damage in the eyes and other organs. Various methods of dialing up ApoM could serve as new treatment strategies for age-related macular degeneration and perhaps some forms of heart failure triggered by similar dysfunctional cholesterol processing.
The study appears June 24, 2025 in the Journal Nature Communications.
Wireless Retina Implant Improves Vision
Stanford University
In a Stanford Medicine-led clinical trial of a wireless retinal prosthesis, people with advanced macular degeneration regained enough vision to read books and subway signs.
The 2-by-2-millimeter chip that receives images is implanted in the part of the retina where photoreceptors have been lost.
The design means patients can use their natural peripheral vision along with the prosthetic central vision, which helps with orientation and navigation.
Of the 32 patients who completed the one-year trial, 27 could read and 26 demonstrated clinically meaningful improvement in visual acuity, which was defined as the ability to read at least two additional lines on a standard eye chart. On average, participants’ visual acuity improved by 5 lines; one improved by 12 lines.
How I Cope with Wet AMD Treatment

Healthline.com, an online health publication, is conducting research for a future article entitled “How I Cope with My Wet AMD treatment”. If you are under treatment for wet AMD and would like to participate in some way, please leave your contact information below and we will forward it to the right party.
The goal of this piece is to offer encouragement and relatability for others living with wet AMD by highlighting a real person’s experience — including how they manage treatment, cope with the emotional and practical challenges of the condition, and what has helped them along the way. This would be a personal narrative, written with care, respect, and sensitivity.
To make participation as comfortable and accessible as possible, there are a couple of ways you could take part. For example, you may choose to write your own story or, if preferred, Healthline will provide questions via email and help shape the narrative based on your responses.
Thank you for your consideration.


Electronic Magnifiers

Technology has made a real difference for those with low vision. Handheld magnifiers have advanced from glass to electronic. Cell phones now offer sophisticated reading applications. Special glasses are giving the visually impaired new mobility.

LVI (Low Vision International) is a Swiss company that designs and manufactures a line of specialized electronic magnifiers for home, school and office.
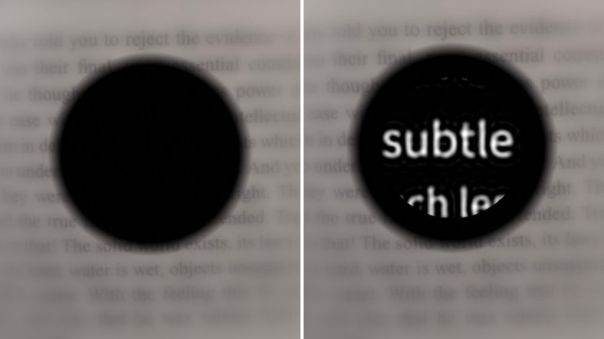
Can Mindfulness Improve Vision?

by Dan Roberts, MDF Director of Resources
Mindfulness means being fully present, aware of where we are and what we’re doing, and not overly reacting or becoming overwhelmed by what’s going on around us. A 2018 study conjectured that relief of chronic stress might be an effective treatment for vision loss. Practicing mindfulness, therefore, may be important to our clinical and home care.
The authors of the study wrote: “The loss of vision after damage to the retina, optic nerve, or brain has often grave consequences in everyday life such as problems with recognizing faces, reading, or mobility. Because vision loss is considered to be irreversible and often progressive, patients experience continuous mental stress due to worries, anxiety, or such as depression and social isolation. While prolonged mental stress is clearly a consequence of vision loss, it may also aggravate the situation. In fact, continuous stress and elevated cortisol levels negatively impact the eye and brain due to autonomous nervous system (sympathetic) imbalance and vascular dysregulation; hence stress may also be one of the major causes of visual system diseases such as glaucoma and optic neuropathy.”
After reviewing recent research, the authors concluded that “stress is both the consequence and cause of vision loss. This creates a vicious cycle of a downward spiral, in which initial vision loss creates stress which further accelerates vision loss, creating even more stress and so forth.”
Doctors and patients, therefore, should be aware of the benefits of stress reduction and relaxation techniques for visual health.
Research Approach at the DeAngelis Lab

While physicians have drugs to treat macular degeneration and are aware of the many risk factors (such as age and family history), there is still a lot about the underlying causes and how the disease progresses that is still unknown. One of the major hurdles that AMD research scientists face is they do not have animal or cellular models that fully represent the complexity of the disease in humans.
The DeAngelis Research Lab, located at the University of Buffalo, approaches this problem by studying actual human tissue. Dr. Margaret DeAngelis is responsible for developing the Utah Protocol whereby donated eyes of all types are collected and preserved within six hours of autopsy. The eyes are then carefully classified and meticulously dissected to isolate just the macula. Further DNA analysis allows them to study the retina at the level of single cells. That, in turn, is helping the scientists at the DeAngelis lab to better understand how AMD develops in humans and to create targeted treatments.
Macular Hole Repair

Dimitra Skondra MD PhD University of Chicago
We have a big study regarding macular hole repair. A macular hole is a very common disorder affecting older patients that may already have macular degeneration. Surgery would be needed to repair the hole. This can cause more eye trauma if the patient has an eye disease.
We have pioneered a new treatment algorithm using drops to close the macular hole. We have six years of data from more than 100 patients that were given the drops. We found that in patients with small holes less than 200 micrometer the drops closed the hole in 70% of the patients and they did not need surgery. The patient population with larger holes did not respond and needed surgery. The success on the smaller holes suggest the clinical trials should continue to bring a safer treatment option to fruition
Metformin and Gut Health

Dr. Dimitra Skondra is the director and leader of the retina microbiome team at the University of Chicago. Her team is investigating the possible protective properties of Metformin in relationship to age-related macular degeneration.
Metformin has been used as an oral medication for type 2 diabetes for more than 30 years. Data was collected from patients that have been on metformin for diabetes or other indications to see if they have less incidence of AMD versus people that don’t take metformin. They found that patients that take metformin have significantly decreased risks for AMD.
The research led to the hypothesis that metformin was improving “gut health” by suppressing inflammatory pathways. This provided a protective element in neovascularization, the cause of wet AMD. Studies suggested many of the properties of metformin for promoting healthy aging and health is by promoting healthy microbiome. Dr. Skondra states, “the best tool we have now to promote healthy microbiome is a healthy diet.
The Impact of Vision Loss on Marriage
by Karen and Dan Leonetti – from an episode of Hadley Presents
My wife was diagnosed with wet AMD in one eye about 4 years ago. She crumbled after the diagnosis. She expected her right eye to go the same way almost immediately and began to grieve for her lost sight even before it actually happened. I didn’t go to pieces immediately, but over the course of the next few months I coped less and less well with the idea of having a “blind” spouse. Even though I read about all the reading aids, etc., I could see how difficult our life was going to be and for a long time could concentrate only on the down side.
Eventually, I was coping so badly that a friend of mine suggested I ask for counseling at the university where I worked. This was a confidential service which he spoke highly of, having used it himself when he suffered a bereavement. What I was going through was also a bereavement of sorts: the loss of a secure future, how bad this could be on our marriage, the many losses to come, etc. The counseling came through, and I slipped away from my office desk for an hour.
I sat down with my counselor and poured my heart out about how low I felt, how bad our situation was. At the start of the second session, my counselor told me that she had Stargardt’s disease. She said she had no central vision and relied on special binoculars to travel to work. However, once at work she got around nicely, thank you. She had studied for her counseling diploma with everyone else, but had her text books transcribed onto audio tapes. She was married and had three children and some grandchildren. She and her husband had just come back from a holiday in Europe, which they had thoroughly enjoyed.
Wake up call! I had no idea from the first session that there was anything different about her at all. I realized this was not a death sentence and not about living in dark rooms and doing nothing with your life. It was about making the most of things, being glad you were alive, and getting on with it.
I can’t say I have fully managed to take all this on board and I know that my wife still has her low days. She has been doing all the right things (anti-VEGF injections, supplements, leafy green vegetables, losing weight) – she does it all, thanks mostly to things we have read and subsequently researched on MDSupport.org. We have totally remodeled our apartment and built in as many vision-friendly changes as we could. Lots of contrast where needed, good and appropriate lighting, etc. We do expect that one day those wavy lines might appear in her right eye. But this time we are armed with lots of education and support. And when the time comes, we will be ready. Most important, we still have each other.
Loss of Self-Confidence

In the early days after my diagnosis, I experienced an unexpected symptom of my chronic vision loss that wasn’t mentioned in anything I was reading about the subject.
My wife, Christina, had been trying to get me to fix our refrigerator’s ice maker for months. This would normally have been a welcome challenge, but after a feeble attempt which took much too long, I gave up.
Our porch light developed an electrical short. A project which used to take me only a few minutes took nearly an hour, and my halfhearted repair would probably not last. Then something happened that forced me to admit that I was starting to give in to my slowly-decreasing vision. I was losing my self-confidence.
It started when I drove to the computer store to get a hard drive for Christina’s computer. I had not been there in quite a while, and the place looked slightly different to me. Everything seemed more askew and unfamiliar, and I had trouble reading the information on the racks. My frustration turned into surliness, and Christina (bless her heart) chose to not take it personally.
The store was out of stock, so we needed to go to a place on the other side of town. When I got back into the driver’s seat, I was feeling a little shaky. Christina had other things to do, so I said I would drop her off at home. She offered to go with me, but I told her it was unnecessary and continued on my own.
As I drove away, I soon became disoriented. This made no sense, because I knew the area. So I drove carefully and paid extra-close attention to my surroundings.
After a while, I began to wonder if I was going the right way, so I decided to pull into a gas station for directions. I turned left at the next intersection, into the wrong side of the median, and ended up facing oncoming traffic. The other drivers shook their heads and rolled their eyes while I inched my way along, and – thanks to one sympathetic lady – I was able to turn across her lane into a parking lot to get my bearings.
I considered phoning Christina – something I had always promised to do in an emergency. But I just wasn’t ready for that yet. She would never feel safe riding with me again, and she would worry even more than usual whenever I would go off alone.
Finally, I found the store. They had what I was looking for, but as I paid for it, I thought, “How am I ever going to install this thing?” A year before, that would never have crossed my mind. But something was happening to me, and it was worse after the past hour of events. I hated that.
Well, it took a good half of the next day, but the installation was a qualified success, and Christina finally had her computer back. So on Monday my confidence had faltered, and on Wednesday it recovered. That’s all I know. I have now given up driving, but I’m still riding an emotional roller coaster. I just want you to know, so that if you are on this same ride, it might help to remember that you have company.
One thing I learned: there is something about this new me that will want to give up when things get tough. But something also gives me the strength to keep trying to be the husband I promised to be. Now I’m going to have another shot at that ice maker.
Breakthrough Research
The Macular Degeneration Foundation is pleased to announce that a team of researchers, funded by the MD Foundation, has made an important breakthrough. It is fully described in the following linked technical article entitled: “A Systems Biology Approach Uncovers Novel Disease Mechanisms in Age-Related Macular Degeneration”.
The science may be difficult for most of us to understand, but the bottom line is clear. This research identifies the genes and pathways that drive macular degeneration. With this essential understanding, the efforts to find effective treatments and one day prevent macular degeneration have received a significant boost.
LINK: Technical Report
Support Groups

Support is something we all need at one time or another. Human beings are social by nature and socialization is necessary for good mental health.
Likewise, trying to keep a problem locked within ourselves is difficult. It is much easier and healthier to “get it out” by talking with others, especially if they have been through the same experience. It may also result in gaining information that will furnish solutions and relieve fears.
Support groups are people who meet face-to-face, by telephone or on-line to share experiences, discuss common problems and seek solutions. Support groups have helped many work their way through the challenges of living with AMD. They are usually free, meet at convenient times, and welcome new members.
What group is best for me? The support group best for you depends on your preferences. Some prefer simple, one-on-one conversations. Others enjoy interacting with a group. If you are computer literate, “Skype”, “Zoom” and “Chat Rooms” may be for you.
Where do I find a support group? First, ask your eye specialist if they know of a group in your town. Second, you may call our Resource Director, Mr. Dan Roberts at 1-816-588-7747. For a complete list of local, state, national and international low vision resources, you may visit https://lowvision.preventblindness.org/resources/ .
Prozac for Dry AMD?
NIH – National Library of Medicine
An antidepressant best known as Prozac could offer the first treatment for macular degeneration according to new research from the University of Virginia School of Medicine.
UVA’s Bradley D. Gelfand, PhD, and collaborators have found early evidence that the drug fluoxetine (Prozac) may be effective against dry age-related macular degeneration. The drug has shown promise in lab tests and animal models. In addition, the researchers were encouraged by the results of examining two huge insurance databases encompassing more than 100 million Americans. That analysis concluded that patients taking fluoxetine (Prozac) were less likely to develop dry macular degeneration.
Based on their findings, the researchers are urging clinical trials to test the drug in patients with AMD. If successful, they believe the drug could be administered either orally or via a long-lasting implant in the eye.
Microcurrent Stimulation
Microcurrent Stimulation is the application of a small electrical current to tissues using electrodes placed on the skin. It has been used for years with FDA approval for the repair of injured soft tissues and for treating muscular-skeletal pain.
Several small studies have applied microcurrent stimulation to macular degeneration. They considered various levels of stimulation, frequencies, pulse rates and ways of applying the stimulation to the area around the eyes. Many have shown promising results with no adverse affects.
A new study in Korea, at the Korea University Ansan Hospital in Seoul, is currently underway. Study subjects will participate in the trial for 16 weeks. If determined to be safe and effective, microcurrent stimulation would be one-step closer to official approval by medical authorities.
A Few Practical Tips
A few easy adjustments to the living areas of a person with low vision can improve visibility and reduce the risk of an injury. Dr. Stewart Shofner of Nashville, TN shares with us 5 practical tips to assist those with low vision.
Lights
Make sure their home is well lit and bright with additional lamps or task lighting. Light switches that are sprayed with “glow paint” show up in the dark providing an extra measure of protection and convenience. Outdoor walkways, kitchen, bathroom and work areas all should be fully and evenly illuminated. Have flashlights nearby in case the power goes out.
Stairs
Mark stairs or slopes with brightly colored tape. Bright colors that contrast with the flooring work best. Handrails are imperative, even if only for a couple of steps.
Declutter
Remove unnecessary household clutter and be sure floors are clear and safe. Offer to help with organizing important items and packing up others to ensure items used daily are easily accessible.
Emergency Numbers
Create a list of important phone numbers in large print on bold-lined paper and program automatic dialing options if available. Include emergency contacts, doctors, family, and closest neighbor’s information near each phone and in the console or above the visor in every vehicle.
Upgrades
Suggest purchasing a large-screen television that produces high-contrast images. Ensure furniture is placed closer to the TV if upgrading is not in the budget.
“The Complement System” – Simplified

We all know that our bodies have an immune system that protects us from infections. A special part of this protection is called the complement system, or just complement.
It was first identified in the late 1800’s as something in the blood of sheep that could be used in humans to treat anthrax.
Today, researchers describe it as a highly complex system that circulates in our blood waiting to be activated. When triggered, complement starts a chain reaction (known as a complement cascade) that attacks foreign and damaged cells by eating them, blowing them up, and hauling them away as waste (not a precise description, but the imagery comes close).
That’s very good news because we rely on it every day to stay healthy. Unfortunately, researchers have discovered that the complement system, which is meant to “complete” or “enhance” the immune system, has the potential to do us great harm.
How the Complement System Can Hurt Us
It is thought that the complement system may actually play a detrimental role in many diseases that involve the immune system. These include asthma, lupus, arthritis, heart disease, multiple sclerosis, the rejection of transplanted organs, Alzheimer’s and macular degeneration.
Poor regulation of the complement system seems to be the problem. Scientists have good reason to believe that two of its ingredients named “factor H” and “C3” can get out-of-whack and do us harm.
Summary
The main role of complement is to recognize and facilitate the removal of waste products (like Drusen in the case of macular degeneration), dead cells, and bad things that invade the body and cause disease.
The complement system needs to be tightly regulated to avoid excessive activation.
Strong genetic links have been made between poor regulation of complement activation in the back of the eye and macular degeneration.Scientists around the world are working hard to develop effective drugs and delivery systems to regulate the complement system. Apellis Pharmaceuticals, for example, has just submitted a New Drug Application to the US Food and Drug Administration for intravitreal pegcetacoplan, a targeted C3 therapy for the treatment of macular degeneration. According to their website, recent studies have provided evidence that pegcetacoplan meaningfully slows disease progression and has the potential to preserve vision longer.
Researchers Study Worms
Using roundworms, the University of Maryland School of Medicine researchers believe they have identified a new and distinct cause of macular degeneration. The discovery offers the potential to identify new ways to treat the disease.

“In order to find a cure for a disease, you have to fully understand what causes it, and we identified potential new contributors that were not known before,” says Bruce Vogel, PhD, Assistant Professor of Physiology and Scientist at the UMSOM’s Center for Biomedical Engineering and Technology (BioMET).
“Our findings suggest that complement factor H plays a role in maintaining the organization of photoreceptor cilia, and this process may be defective in age-related macular degeneration,” says Vogel. “We plan to continue this work to determine how this structural disruption affects vision and to determine whether we can reverse the disruption and restore photoreceptor function.”
Pegcetacoplan Study Results

Press Release
WALTHAM, Mass., March 16, 2022 (GLOBE NEWSWIRE) — Apellis Pharmaceuticals, Inc. (Nasdaq: APLS), a global biopharmaceutical company and leader in complement, today announced longer-term data from the Phase 3 DERBY and OAKS studies, which showed that intravitreal pegcetacoplan, an investigational, targeted C3 therapy, continued to reduce geographic atrophy (GA) lesion growth and demonstrate a favorable safety profile at month 18 for the treatment of GA secondary to age-related macular degeneration (AMD). These data will be included in the New Drug Application (NDA) that the company plans to submit to the U.S. Food and Drug Administration (FDA) in the second quarter of 2022.
“It is exciting to see these positive data with pegcetacoplan, which showed continuous and potentially improving effects over time. These 18-month results provide further evidence that pegcetacoplan meaningfully slows disease progression and has the potential to preserve vision longer,” said Jeffrey S. Heier, M.D., principal investigator of the DERBY study and director, retina service and director, retinal research, Ophthalmic Consultants of Boston. “In my practice, I have seen how devastating it can be for people living with GA to lose more of their vision year after year. There is an urgent unmet need in GA, and these results reinforce the potential of pegcetacoplan to become the first-ever treatment for patients with this debilitating disease.”
New “Wet” AMD Medication Delivery System
The FDA has approved Roche’s Susvimo (ranibizumab), a long-lasting injectable drug for treating people with “wet” age-related macular degeneration.
Susvimo, which continuously delivers therapy via a refillable ocular implant, can be administered just twice a year, providing an alternative to other injections that are often given monthly.
The drug’s approval was supported by phase 3 data demonstrating that patients treated with Susvimo experienced vision increases equivalent to those receiving monthly ranibizumab injections. Roche noted that 98 percent of patients were able to go six months before needing their first refill of Susvimo.
Additional Information
Chocolate!

In recent years at least two studies demonstrated the benefits of flavonoid-rich dark chocolate over milk chocolate as to improved vision. That was good news for chocolate lovers.

In a new double-blind randomized clinical trial (Department of Ophthalmology Ludwig-Maximilians-University, Munich, Germany), the short-term benefits of dark chocolate were once again put to the test.
Unfortunately, this time they saw no benefit to visual function of either dark or milk chocolate. Researchers admit sample size was small (22 participants) and further trials would be needed to rule in or out possible longterm benefits.
Conclusion: Chocolate tastes good!
Why We Should Learn About the Side Effects of Drugs

By Dan Roberts – MDSupport.org
“Tom”, a 73-year-old male, complained of severe dry eye syn- drome and loss of acuity after one injection of an anti-VEGF drug for treatment of wet macular degeneration. Tom had previously undergone four months of treatment with a similar drug, but his physician recommended changing to the newer and less expensive one.
Both drugs had been clinically-tested and FDA-approved for ophthalmic use. Dry eye syndrome was not reported in the trials as an adverse event for anti-VEGF drugs, so the physician did not suspect it to be related. Instead, he prescribed medication to treat Tom’s new symptom. Tom refused the medication, saying he felt that his condition may be an adverse event so rare that it was not reported in the trial results. He did not agree with his physician’s opinion that the benefits of the new drug outweighed the risk in this case, and he insisted that he be returned to the original treatment. After doing so, Tom’s condition improved, and his vision returned to baseline.
Agencies such as the FDA are responsible for approving drugs and for monitoring their safety after reaching the market. Timely and accurate reporting of side effects and serious adverse events (SAE’s) by pharmaceuticals and physicians is important, especially in the case of newly marketed drugs. Physicians are expected to report to the pharmaceutical companies, and the companies are expected to take appropriate action when necessary. The safety of the public depends upon compliance with reporting procedures. Unreported SAE’s, however, are still too common, and can lead to public health disasters. Physicians and pharmaceutical companies are obliged to comply with the reporting process, and patients play an important role as well. Every patient should be aware not only of the pre-market discovery of side effects and SAE’s of a particular drug, but of the potential for new and unexpected events.
Patients should be encouraged to report all physiological and psychological changes during treatment, whether or not such changes are reported in the trial results and discussed in the prescribing information. Such reports should be made to the physicians, but in the event that a report goes no further, patients need to have the opportunity to communicate directly with the drug companies and governing agencies, and to share information with one another.
An Internet site at http://www.eHealthMe.com is one solution. The site has an interactive database for use by patients to identify, track, and report their individual side effects and adverse events during drug therapy. The web-based application contains a searchable database of labeled side effects, SAE’s, and warnings for individual drugs on the market. Additionally, the application allows patients to anonymously enter information and communicate with one another about personal conditions not listed.
The newly-entered information is tabulated by drug, type and frequency, and the results are accessible to physicians, pharmaceutical companies, and governing agencies. The intention is that this complement to the reporting process might expedite discovery of new post-market side effects and SAE’s, allowing for more immediate and effective intervention when necessary. To make a report, go to http://www.eHealthMe.com
Life-Style Changes
Through a program of diet, sleep, exercise, and relaxation techniques, combined with supplemental probiotics and phytonutrients, a team of 3 international scientists have described a plan that may actually reverse aging and its resultant effect on disease.
In their study, the diet and lifestyle treatment group decreased in biological age by 3.23 years compared to the control group. The data also showed that those in the treatment group decreased in biological age by 1.96 years over the eight weeks.
Some of the important life-style changes:
- Include the most colorful fruits and veggies in your diet
- Include fiber and probiotics for “gut health”.
- Quit smoking.
- Sleep, exercise and relaxation techniques can lower
blood pressure which, in turn, can lower a patient’s
intraocular pressure
“Smart Phones – Getting Better”
Joe Fontenot MD
Patti Hacker Equipment Specialist
Community Services for Vision Rehabilitation
Smart phones are used by a majority, possibly more than 75 %, of the US population. There are literally thousands of “Apps” or Applications for the blind and visually impaired. More and more are multifunctional and many are free. For the blind and visually impaired, the smart phone is the best thing since Louis Braille’s tactile alphabet. It allows them to communicate effortlessly, do research and have a hand-held computer. More apps are being developed every day, and thousands are now available. Many are useful for the visually impaired, and some are specifically for them.

There are many different makes and varieties of smart phones, and some are simplified and advertised as designed for easy use by the visually impaired. At this time in 2021, the iPhone is the most popular in the US, including in the blind/visually impaired population. In some other countries, the Android may be more popular. Phone costs vary , and at this time in the US, the I Phone is usually a few hundred dollars more expensive than the Android models.
The iPhone
Since being introduced in 2007, the IPhone by Apple has been regarded by many as the best smart phone for the visually impaired. This is primarily because it has many built-in accessibility features, which simply need to be turned on in Settings such as “Voiceover” which will read the screen display, and “Zoom” and other magnification options.
Apps for the Visually Impaired
In addition to the inherent accessibility options in the IPhone and the Android, there are now a myriad of apps. These will magnify, contact help from a sighted volunteer, count money, recognize faces, etc. The variety and usefulness of apps has steadily and progressively improved, and there does not seem to be an end in sight.
As an example, we can look at apps for reading text. In 2007 a text reader app, the Kurzweil NFB reader app was introduced at a cost of $99. Subsequently the A few years later, another text reader app, Envision reader was available at $20. In 2020 the Apple Seeing A1, which in addition to reading text will count money, has a bar code scanner and identifies images was released and it is free for iPhone users.
This sort of increasing function and decreasing cost is typical of app development for the visually impaired, and we hope will continue.
All with vision loss should use smart phones to their maximum and will become more independent, functional and happy because they do so.
Summary
The smart phone is a communication and computing device of great help to all, especially for the visually impaired. It is rapidly improving, and more apps that are specifically for the visually impaired are becoming available almost weekly.
What Do I Do? … My Doctor just told me I have Macular Degeneration
Most people found to have AMD are:
- Over the age of 55
- Have noticed changes in their vision
- Have gone to an ophthalmologist or optometrist who found evidence of macular degeneration in their eyes.
Dry AMD
Some of the initial changes to the eye caused by AMD are mild and do not require treatment. Your doctor will see small yellow areas of “drusen”, a German word for “bump”, in one or both eyes. This is known as “Dry Macular Degeneration”. Symptoms may include visual distortions, the need for more light when reading and a blurry or blind spot in your central field of vision. Side (peripheral) vision is not affected.

Wet AMD
The “Wet” type of macular degeneration is characterized by the growth of abnormal blood vessels that leak fluid or blood into the macula (the area of the retina responsible for central vision). Symptoms of wet macular degeneration are the same as the dry form but usually appear suddenly and get worse rapidly.
What to Do!
Ask your eye doctor if you should see an ophthalmologist who specializes in the treatment of macular degeneration or a retina specialist. Retina specialists are best qualified to decide if active treatment is needed and when to begin therapy.
Treatment for the active form of age-related macular degeneration is currently an injection of an “anti-vascular endothelial growth factor”, or “anti-VEGF”, into the eye. Injections may be repeated at 1 to 3 month intervals for some period of time depending on the response. Although this sounds painful, it is not … and very few people stop getting the shots because of discomfort.
Don’t Stop!
DO NOT PANIC or stop doing all that you need or want to do. Continue your job and hobbies! Vision Rehabilitation has training, techniques and devices that allow even those with severe vision loss to continue to function as they always have. From simple stronger glasses to advanced electronic devices, much help is available. Developments in technology in the last few decades have made this easier than ever. Ask your doctor for a referral to a low vision rehabilitation clinic. You will be glad that you did!
Summary … “What Do I Do?”

- If you are a smoker, STOP! Smoking increases the chances of continuing “active” AMD with bleeding and vision loss
- See your primary doctor for control of blood pressure, cholesterol and general health
- Exercise. Ask your primary doctor about this.
- Eat a diet rich in green leafy vegetables.
- Consider taking vitamins. There are some preparations specifically for people with ARMD. Ask your eye doctor about this. There are guidelines and the vitamins are high in antioxidants.
- When outside, wear sunglasses with UV and blue light protection and a hat with a visor or broad brim.
- If your vision is affected, see a vision rehabilitation specialist or clinic
- If your eye doctor advises, look at an Amsler grid. (see MAGNIFIER Issue #117 for details).
- See your eye doctor and retina specialist as often as advised or sooner if your vision changes
Joe Fontenot MD, CLVT
Medical Director, Community Services for Vision Rehabilitation – 600 Bel Air Blvd, Suite 110, Mobile AL 36606
5 New Treatments on the Horizon
Newest Sustained-Release Anti-VEGF Drug in Trials
EyePoint Pharmaceuticals, Inc. announced on January 28, 2021 that the first patient has been dosed in their Phase 1 clinical trial of EYP-1901. EYP-1901 is a potential twice-yearly sustained delivery intravitreal anti-VEGF treatment for wet age-related macular degeneration (wAMD). It is the newest of several sustained delivery drugs under study, this one promising to extend treatments from 4-6 weeks to only twice a year.
Faricimab for Wet AMD Effective at 16-week Intervals
Genentech has announced positive topline results from its Phase III studies, TENAYA and LUCERNE, evaluating its new drug faricimab for people with wet (neovascular) age-related macular degeneration (nAMD). Both studies have shown that people receiving faricimab injections at fixed intervals of up to every 16 weeks achieved visual acuity outcomes as effective as those receiving injections every 4-6 weeks.
Zimura Shows Significant Suppression of GA
(late stage dry macular degeneration)
IVERIC bio, Inc. has announced positive Phase 3 results from its GATHER1 clinical trial with Zimura (avacincaptad pegol). Zimura® inhibits complement factor C5, which is believed to be involved in the development of AMD. The reduction in the mean rate of geographic atrophy (GA) growth over 12 months was better than 27% group as compared to sham control groups. The data was statistically significant, and the drug was generally well tolerated. GATHER2 is currently underway to further evaluate the efficacy and safety of Zimura in patients with GA.
Lucentis Substitute In Phase 3 Trials
Samsung Bioepis is reporting first year results from their phase 3 study of a proposed lucentis biosimilar (SB11). A biosimilar is a biological product (derived from a living organism) that shows no clinically meaningful differences from another biologic (eg. Lucentis). This study has shown that, at 52 weeks, primary end points were met for visual acuity and retinal health, suggesting that it could become a substitute for Genentech’s Lucentis (ranabizumab). This would be the first biosimilar for an anti-VEGF drug, which could lead to significant cost savings for the U.S. health system and consumers.
APL-2 Slows Progression of Early Disease in Patients with Geographic Atrophy
Apellis Pharmaceuticals,Inc. announced their analysis of the Phase 2 FILLY study investigating intravitreal pegcetacoplan (APL-2) for the treatment of geographic atrophy (GA), also known as advanced dry macular degeneration. The post hoc analysis found that the monthly treatment reduced the rate of progression to GA by 39 percent in areas of the retina outside of existing GA lesions.
APL-2 is the only targeted C3 therapy in Phase 3 clinical trials for GA, which affects approximately five million people globally and has no approved treatment. According to SriniVas Sadda, M.D., President & Chief Scientific Officer of the Doheny Eye Institute and lead investigator, “This study provides exciting evidence to support further exploration of the potential of pegcetacoplan for earlier intervention in the course of GA.”
Watch Exclusive Research Video’s Produced by the MD Foundation

